A man wearing a face mask bicycles along Broad Street, Wednesday, Nov. 18, 2020, in Philadelphia.
Matt Slocum / AP Photo
A man wearing a face mask bicycles along Broad Street, Wednesday, Nov. 18, 2020, in Philadelphia.
Matt Slocum / AP Photo
Matt Slocum / AP Photo
A man wearing a face mask bicycles along Broad Street, Wednesday, Nov. 18, 2020, in Philadelphia.
Earlier this week, Philadelphia became the first major city in the country to reinstate an indoor mask mandate. Many local residents — and even some public health experts — questioned the decision, since COVID-19 case rates in the city are still lower than or similar to many neighboring areas that have not yet brought back similar precautions.
But the decision wasn’t much of a decision at all — it was automatically triggered once case rates surpassed the threshold outlined in Philly’s risk measurement system, which the city’s public health department calls its “Response Levels.”
Is Philadelphia’s criteria for precautions too sensitive? Or, is the city setting a model for the rest of the country?
How Philly’s response system stacks up against the CDC’s
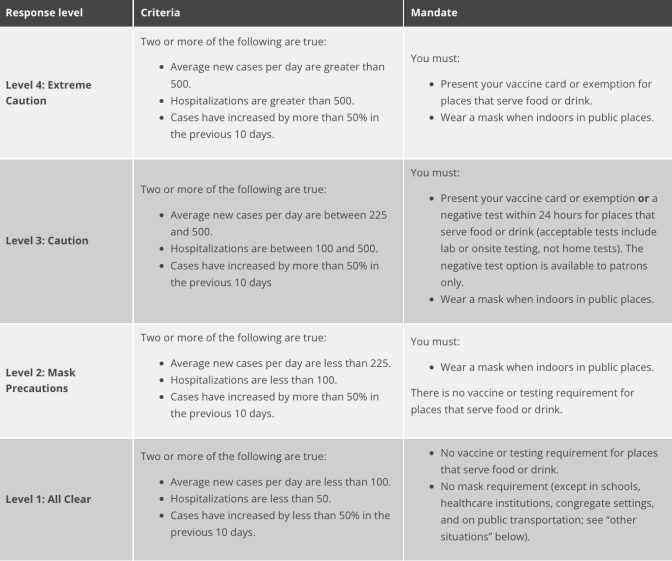
Philadelphia’s indoor mask mandate goes into effect on Monday, April 18, and will apply to restaurants, gyms, offices, and schools. Establishments can choose to require proof of vaccination in lieu of masking.
Philly’s system for measuring COVID risk has four categories, ranging from “All Clear” to “Extreme Caution.” As case rates and hospitalizations rise, more precautions are triggered.
Philly’s system is stricter than the one developed by the Centers for Disease Control and Prevention, which was released in late February. The CDC’s system doesn’t recommend masks until its highest risk level, and it uses hospitalizations, more than cases, to measure that risk.
CDC Director Rochelle Walensky explained the shift from cases to hospitalizations by saying that the main goal now was to prevent serious illness, death, and a strain on our nation’s health care systems, making hospital capacity the most important thing to keep an eye on.
However, many experts question whether that should be the only goal from a public health perspective, and say that it’s still important to count cases. Since hospitalizations can lag weeks behind rising case counts, they’re not a helpful tool to get out ahead of a wave and prevent more infections.
“It’s like instead of using a weather forecast, it’s just putting a bucket out and seeing how much rain is in it,” said epidemiologist Michael Levy, an associate professor at the University of Pennsylvania.
He argued that Philadelphia’s stress on case counts is important to prevent transmission. The city’s number of COVID cases is likely a vast undercount, considering that many residents are testing positive at home.
And there are important reasons to prevent the spread of infection. There’s still a lot we don’t know about how COVID interacts with other diseases, or its long term effects. Plus, argues Abraar Karan, an infectious disease physician at Stanford, the public’s idea of what constitutes an “acceptable” level of disease might be skewed. We don’t want to be in the habit of tolerating so much illness, he said.
“We are so traumatized by early 2020 and mid-2020 that our standard for what we are deeming acceptable or successful, I think, is still too low,” he said.
Flexibility vs. transparency
Levy acknowledged that Philadelphia’s decision to create a tiered “Response Level” system came from a place of wanting to provide clarity. But, he said, the automated system — and similar ones like it — removes the ability for public health officials to exercise their judgment. He said he thought color-coded risk systems were usually failures, citing both the terrorism alert tiers developed after the September 11 attacks, as well as Pennsylvania’s color-coded pandemic reopening system.
Both systems fell victim to typical pitfalls of automated schematics, said Levy. In the case of the terrorism advisory system, the country was on high alert for so long, that the designation became meaningless. And in the case of Pennnsylvania’s reopening code, the goal posts for when the counties would qualify as “yellow” or “green” kept changing.
“It’s easy to paint yourself into a corner, and that’s something that I think everyone’s trying to avoid,” he said
Levy said he preferred relying on the expertise and clear communication of health officials, the same way you would for a weather forecaster. He gave the example of a snow day — a designation that has no specific set of metrics attached to it.
“It’s always kind of a bit of a judgment call based on forecast and based on the actual accumulation,” he said. “The combination of a bit of expertise and a lot of common sense.”
But Jennifer Kolker, a professor of health management at Drexel University, said people are sick of relying on the word of public health officials, and have reason to be distrustful after two years of death and disease. She said having a clear and consistent system is good for engendering public trust.
“Public health needs to be credible and the way you achieve credibility in large part is through transparency and trust,” she said. “People want to know ‘why.’ So, simply saying, ‘Oh yeah, a bunch of talking heads got in a room and we decided masks on, or masks off,’ that pisses people off, and for good reason,” Kolker said.
For its part, the city claims its “Response Levels” can be both clear and responsive.
“Rather than picking an arbitrary date to start or end mandates, we chose a responsive system that allows our response to be only as strict as it needs to be, but not unsafe,” wrote James Garrow, a spokesperson for the city’s health department, in an email. “Because the pandemic has proven to be so unpredictable, this system allows the city to adjust its protection levels in real time as the virus surges and falls.”
The three experts stressed that there is no perfect point for a city or state to reinstate precautionary measures during this pandemic — it’s always a bit of a guess and a moving target. But the longer you wait, the less successful they’re likely to be at preventing a surge of infections.
The tricky thing about prevention measures is that it’s hard to show that they have worked, because you’re measuring something that didn’t happen. And it can be hard for health officials to make the inconvenient things they are asking people to do feel worth it, when all they have to show for it is a less bad outcome.
“Public health’s job is to protect the public’s health in the least restrictive ways possible,” said Kolker. “We don’t lock people up with tuberculosis anymore, right? We used to just lock people up, then you’d have no spread, but then we realized you can’t just do that. So we come up with other ways.”
Kolker and Karaan both agreed that in theory, masks are an individual-level intervention that ideally would be reserved as a last resort. But absent comprehensive infrastructure solutions, such as enhanced ventilation systems in all buildings and ways to measure indoor air quality, those individual-level solutions are what we’re left with.
And until we have those engineering technologies better developed, along with easily accessible COVID treatments and a better understanding of the long-term effects of the disease, the experts said that masking indoors when cases rise shouldn’t be too much to ask to protect the public.
Sometimes, your mornings are just too busy to catch the news beyond a headline or two. Don’t worry. The Morning Agenda has got your back. Each weekday morning, host Tim Lambert will keep you informed, amused, enlightened and up-to-date on what’s happening in central Pennsylvania and the rest of this great commonwealth.