Matt Rourke / AP Photo
Matt Rourke / AP Photo
Matt Rourke / AP Photo
(Philadelphia) — Many immunocompromised people and their physicians are concerned that the COVID-19 vaccine might not protect them to the same degree it protects others.
Some studies predict that after getting the Pfizer or Moderna vaccine, immunocompromised people have 75% protection against symptomatic COVID-19, compared to 94% for others.
A few weeks ago, the Health Desk Help Desk reported on the vaccine’s effectiveness among those who are immunocompromised. Since then, we’ve received more questions about specific conditions and concerns, so we reached out again to the medical experts.
In clinical trials so far, the effectiveness of the vaccine has correlated with the production of antibodies. That doesn’t mean antibodies are the only function involved in a person’s protection from the coronavirus, but so far the research finds that it’s the strongest correlation.
Antibodies are made by B cells. But some health conditions, such as certain cancers and chemotherapies, reduce that arm of the immune system. Prescription drugs that treat some autoimmune diseases, such as multiple sclerosis and certain rheumatological diseases, also eliminate B cells.
Physicians also are concerned about transplant patients, who are immunosuppressed to prevent the body from rejecting the new organ.
While studies show many immunocompromised people don’t produce high levels of antibodies after getting the vaccine, it’s important to note that experts don’t yet know if antibodies are the only correlate to vaccine effectiveness, nor what percentage of antibodies is needed. Researchers are trying to determine whether other arms of the immune system, like T cells, can also protect people from coronavirus. T cells work once a virus starts to infect a few cells, and should be able to eliminate the virus from those cells.
“I think that we are all incredibly understanding of how difficult this moment is in fully understanding whether our patients are protected or not and whether they can resume their normal lives,” said Dr. Marcus Pereira, an infectious disease specialist at Columbia University Vagelos College of Physicians and Surgeons and an expert on infectious complications in transplant patients.
“Studies are ongoing and we’re going to get the information needed to protect our patients,” Pereira said. “It might not come readily, and I think there will be some degree of anxiety and frustration, but it’s coming.”
Jill Kaiserman from Wayne asks, “I was diagnosed with ovarian cancer in September 2020. Finished chemo in February and received my second shot of Moderna in April. Is my immunity lower than those who are healthy?”
Most cancer patients, especially those with solid tumors — as opposed to lymphocytic leukemia, for example — do have a reasonable response to the vaccine, said Dr. John Wherry, director of the Institute for Immunology at the Perelman School of Medicine at the University of Pennsylvania.
Chemotherapy, however, is generally an immunosuppressive treatment and can have consequences for several months. So it is possible that a person’s vaccine response might be diminished compared to that of other people. But in comparison to other types of cancer, or other types of immunocompromised situations, the suppression of the immune system for an ovarian cancer patient is not as severe, Wherry and Pereira said.
It all depends on a person’s treatments, disease status, and overall health.
“I think the best advice I can give is that your vaccine response may be more related to overall health. If you’re not currently on chemotherapy, you’re likely to make a reasonable response. But it’s worth talking to your physician, your oncologist, or your primary care physician about whether you can get an antibody test to see if you have antibodies,” Wherry said.
Not all cancer treatments are the same, he added. “So unfortunately, the devil’s in the details.”
As far as chemotherapies go, physicians are particularly concerned about rituximab, which is not that toxic an agent but essentially destroys all the B cells. Other chemotherapies have less impact on the immune system.
“Rituximab, for example, you have a six-month duration in terms of its impact. So that’s going to be a big problem. [But for other treatments], probably after a few months, the immune system should reconstitute itself,” Pereira said.
Either way, he said, it’s important to get the COVID-19 vaccine because any protection is better than no protection.
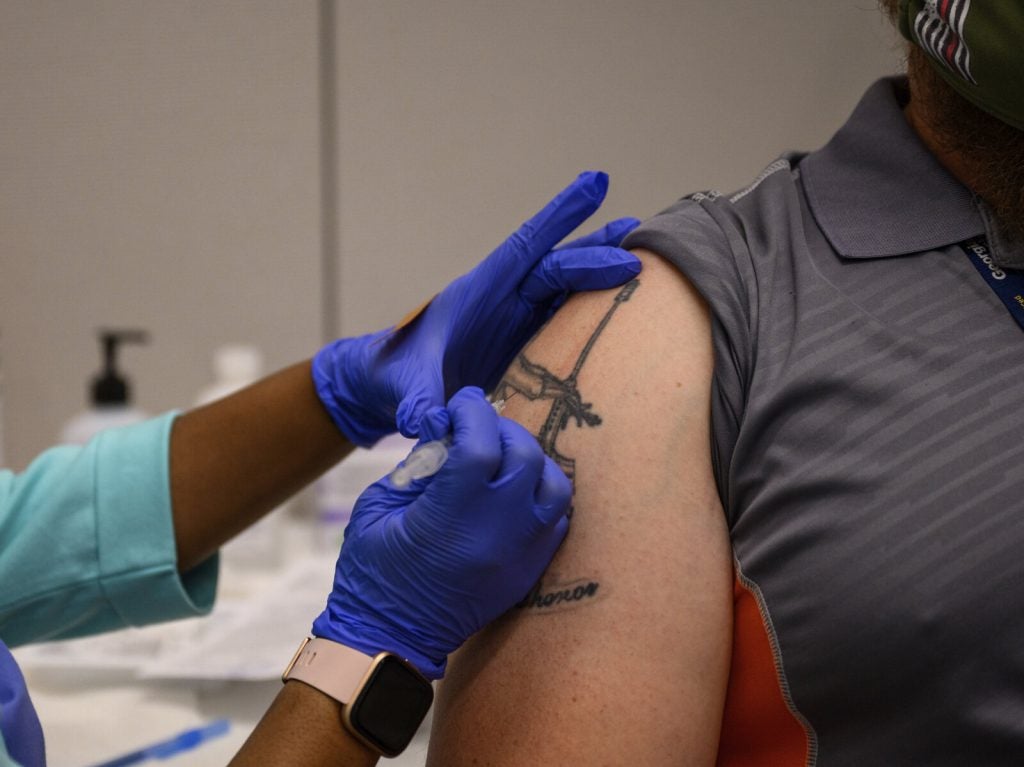
A Georgia Tech employee receives a Pfizer coronavirus vaccination on the campus on April 8. (Danny Karnik/AP)
This question came in from Bucks County: “Are all liver transplant patients compromised to the same degree?”
Transplant patients get a variety of immunosuppression treatments, which can depend on the kind of organ transplant performed. Both Wherry and Pereira said liver transplants tend to be accepted a little bit more readily than kidney or lung transplants.
“Not all liver transplant patients receive the same high degree of immunosuppression as, let’s say, kidney transplant patients do,” Wherry said. “It’s hard to talk in absolutes, because every patient is different. But it may be that there are some liver transplant patients that are less immunosuppressed.”
Pereira said that within the first six months to a year, transplant patients are heavily immunocompromised because of the initial therapies and because they’re still recovering from the surgery. That’s usually the period in which they’re most vulnerable to infections, he said.
After a year or two, there is somewhat of a reconstitution of the immune system, Pereira said. The immune system of patients five or 10 years out from a liver transplant — in the absence of complications like treatment for rejection — is somewhat restored.
“What we have seen in terms of antibody responses after the vaccine or even after natural COVID-19 infection is that patients many years out from a transplant generally have a better response than those who are more recently transplanted — that translates into liver transplants as well,” Pereira said.
“Actually, if you were to compare liver transplants versus kidney, heart, and lung transplant recipients, liver transplants are less immunosuppressed and generally have a better response to these vaccines than other groups.”
An audience member from Delaware County asks: “I have a compromised immune system due to persistent Lyme disease. Will this have a bearing on the vaccine?”
Persistent Lyme disease is not well understood immunologically, Wherry said. But both he and Pereira said they did not expect that Lyme disease itself would alter a person’s response to any vaccine, though more research is needed to say definitively.
“The simple answer is, I don’t know. I think, again, it’s possible in at least some settings to see if you can get your antibodies tested clinically,” Wherry said. “If you have made normal responses to other vaccines, like the yearly flu vaccine, I think you can reasonably extrapolate from that to think that you’ll make a productive response to the coronavirus vaccine.”
David Barry from Princeton wrote WHYY News to say: “I’ve seen people who are immunocompromised and the Pfizer 2-shot treatment did not produce antibodies, so they got a 3rd J&J and saw a jump in antibodies. I’m a kidney transplant and just concerned about side effects from a third shot.”
It’s an important question that the entire transplant community is trying to address right now, Pereira said.
Operation Warp Speed was incredibly successful at developing and authorizing effective and safe vaccines quickly, he said. But one of the downsides was that immunocompromised patients, including solid-organ transplant recipients, were not included in the initial trials. Physicians were left with little guidance in terms of what their transplant patients should expect from the vaccines, both in terms of safety and, more importantly, in terms of efficacy, Pereira said.
That led to studies of antibody responses among transplant recipients after the first and second doses of the mRNA vaccines (Pfizer and Moderna). Some studies show that solid organ transplant recipients only have 3% to 58% antibody response. Kidney transplant recipients, in particular, have one of the lowest response rates in comparison to the other solid-organ transplant recipients.
Those results came in about the same time that the Centers for Disease Control and Prevention released guidelines for fully vaccinated people permitting them to participate in most activities without masks and physical distancing.
“We were left as a community to try to figure out if that applied to our patients in light of that data of reduced antibody response,” Pereira said.
It’s a complicated issue. Physicians still don’t know whether the production of antibodies is the only reason why the COVID-19 vaccine is effective. There are several other immune correlates that could help someone fight the coronavirus: B cells create antibodies; T cells can kill bacteria or viruses; and cellular immunity kills foreign invaders.
And there’s also debate about the best way to measure someone’s antibody levels.
“I think everybody agrees that the CDC recommendations likely don’t apply to our patients. But recommending measurements of antibodies has been hugely controversial. And that’s because essentially, what you do with that result has been really up in the air,” Pereira said.
“So you can imagine a situation where a kidney transplant patient gets a result after they’re fully vaccinated and can get a spike antibody result. If it’s positive, are we going to be confident enough to tell that patient, ‘You are immune, you go ahead and follow the CDC guidelines, despite you being an immunosuppressed individual, based on this one antibody test?’ I think many providers would say, ‘Hold on, let’s not say that you’re fully protected. You should probably still wear a mask and practice social distancing and be safe,’” he said.
“And if you then imagine a patient getting a negative antibody response to the vaccine, how would we interpret that? I think that many would say, ‘OK, well, it seems that you’re probably not protected, continue to wear a mask, and practice social distancing and stay safe. The CDC recommendations don’t apply to you.’ So in some ways, the controversy has been that most providers have said, whatever the result is, the recommendation is going to be the same.”
The French Ministry of Health recently recommended a third dose for immunocompromised patients, finding that it could boost their antibodies.
There have been some preliminary studies in the United States. A Johns Hopkins study found that third doses benefited a small number of patients who were immunocompromised. Data published last week in the New England Journal of Medicine showed that after the second dose of the vaccine, immunocompromised patients had a presence of antibodies at 40%, but after getting a third dose, that antibody response increased to 68%.
No official recommendation has been made in the U.S., however. Pereira and Wherry predicted that there will likely be a recommendation for a third dose in the U.S. at some point, but that more research is needed. The topic was discussed at a meeting of the CDC’s Advisory Committee on Immunization Practices last week. But more research is needed before the group makes any recommendations.
Wherry said the risk associated with a third dose is relatively low for immunocompromised people in general.
“These vaccines are pretty safe, especially in these patient groups,” he said. “But I think it’s something worth discussing with your physician … there is some precedence and some, again, anecdotal reports of an increased likelihood of generating antibodies after a third dose in patients who are immunosuppressed.”
Pereira added that there are some concerns for transplant recipients, however. The more a person is vaccinated, the more the immune system is stimulated. For solid-organ transplants, stimulating the immune system is not always safe because it can lead to rejection of the organ, which can be serious.
“So you really have to be very careful about these things. And really what we have to go about is really doing the research and not necessarily having patients on their own getting a third dose,” Pereira said.
Mark Halpern from Conshohocken asked: “I had the Moderna vaccines and then had a negative SARS CoV-2 IgG antibody test. I am 74 [years old] with diabetes 2 and survivor of prostate cancer and radiation. What should I do next?”
The COVID-19 vaccines are very effective, but they’re not 100%. Moderna is 95% effective, which means the vaccine doesn’t work in five out of 100 people. There are a variety of reasons why a vaccine might fail an individual, Wherry said.
“Perhaps, when you got the injection, the needle didn’t go deep enough and wasn’t in the muscle, and so the vaccine didn’t, what we call, ‘take’ effectively. It may be something related to a person’s immunological history, in this case due to diabetes or previous cancer treatment, or it may just be something that we don’t understand yet,” he said.
Antibodies also can manifest late.
“We do see that occasionally in other settings, where the immune system is a little bit slow and it takes a little while to really get going,” Wherry said. “So it’s worth doing another antibody test for sure. If that comes up negative, I would talk to your physician about possibly getting a third dose of the same vaccine or crossing over to another vaccine platform like J&J.”
Continue to wear a mask and practice social distancing, Pereira said. He added that it’s also important to note there are dozens of commercial assays, and not all of them measure antibodies in the same way.
“So it’s really important to obtain the right tests to even begin to understand vaccine response,” Pereira said.
“And for that individual, I think that particular category of a cancer survivor, they are probably going to be in that group that may benefit from a booster vaccine, much like other cancer patients or those actively on chemotherapy or solid-organ transplant patients. But I think we still need to do the research and determine that. And I think that the CDC and other agencies are actively looking at that right now.”
Another WHYY audience member told us: “I was diagnosed with CLL [chronic lymphocytic leukemia] over eight years ago. I took the Pfizer vaccine second shot in February and then took the spike antibody test a few weeks ago. I have no antibodies and wanted to ask about the options I may have.”
It’s very common for CLL patients to demonstrate a significantly reduced response to the vaccine. Wherry said physicians are discussing a number of options, including a third dose, and an infusion of antibodies — though he said it’s not yet available for most patients.
Pereira also recommends this individual practice social distancing, continue to wear a mask, and ensure that those around are vaccinated.
“The issue of CLL, and perhaps that also speaks to solid-organ transplant recipients, is that one of the problems may be as we begin to study responses to a third dose, is that a third dose may also not be sufficient, and that actually might be a problem in particular with patients with CLL — they may get sort of a slight boost in their immune response, but it may still not be sufficient,” he said.
“So we really have to study this very carefully. And we know from precedent in other vaccines, for example, the hepatitis B vaccination among patients who are immunocompromised, sometimes they need four or five doses until you get some response.”
First and foremost, physicians need to understand what measurement of the immune system is needed to know if a person is protected from COVID-19, Pereira said.
There are not enough studies yet that explain that, the experts said. There are also dozens of commercial assays available, and each has its own curve in its numbers, Pereira said.
“And some of them are difficult to interpret, and definitely they’re very difficult to compare across the board. So it’s highly dependent on the assay. And you can see that even in the studies that are available out there, that, some studies, for example, they’re all using different spike antibody assays. If I had a test and if I were to look at whether I had the adequate response or not, I would look at that particular test characteristics and speak with their provider about whether the number that you get is related to a good response or not a good response.”
“I am immunocompromised due to Rituxan maintenance therapy for non-Hodgkin’s lymphoma,” another audience member said. “I’ve heard about gamma globulin being infused with COVID antibodies and then given to patients who are on monthly infusions of gamma globulin. What can you tell me?”
Gamma globulin replaces what a patient is missing. Over time, as vaccination numbers increase, gamma globulin — which is basically a pool of antibodies from healthy donors — will start to contain antibodies to COVID-19. So it’s possible that it will become an effective strategy to help boost immunity for those who can’t generate it themselves, Wherry said.
Monoclonal antibodies have been used as a treatment for COVID-19 patients to prevent severe disease. Now, researchers are studying whether monoclonal antibodies can be used to prevent people from contracting the virus in the first place.
“So we have asserted that there’s some debate now about, for these immunocompromised individuals who we don’t think are responding to the vaccine, whether they should get periodic monoclonal antibodies, whether it’s once a month or once every three months, it really depends,” Pereira said.
But that option is not yet available for most patients, the experts said.

An Eli Lilly researcher tests possible COVID-19 antibodies in a laboratory in Indianapolis. (David Morrison/AP Photo)
“I have Bordetella bronchiseptica [a common pathogen in the respiratory tract of many wild and domestic animals, rarely found in humans], on regimen Tobramycin inhalation 28 days on, 28 off. Have rheumatoid arthritis, [and am on a] monthly infusion Orencia. Now diagnosed with CLL, awaiting what stage of disease. Do the above drugs affect B & T Cells?”
Wherry recommended that this individual talk in detail with his or her physician.
The antibiotics for Bordetella are unlikely to affect the immune response, he said, but the bordetella infection itself may.
The experts said autoimmune diseases somewhat affect vaccine response, but not to the degree cancers that affect the blood, bone marrow, and lymph nodes, or solid-organ transplants do. It is possible medication for rheumatoid arthritis could affect vaccine response, but more needs to be known.
“We don’t yet know a lot about how immunosuppression for RA and other diseases affect vaccination,” Wherry said. “There’s some data starting to emerge, and most people seem to make at least some immune response to the vaccine. We don’t yet know how protective those responses will be, but people do respond to the vaccines.”
The treatment for CLL may be more immunosuppressive, however. So this person should be sure to get vaccinated before starting that treatment, Wherry said.
“I suffer from psoriasis and am currently taking Otezla orally to control my outbreaks. I recently learned that folks who take immunosuppressive medications may not produce any or sufficient numbers of antibodies against the COVID-19 virus. I am curious if you have learned if PDE4 medications (i.e. Otezla) present similar issues as TNF [a medication for autoimmune conditions that block a substance in the body that can cause inflammation and lead to immune-system diseases].”
There are many different flavors of immunosuppressant drugs, and they treat a variety of different manifestations of autoimmunity or other diseases, Wherry said. The metaphor he uses is getting work done on your car.
“The ones that we have looked at so far are the equivalent of taking the engine out of the car. They hit the big parts of the immune system so that you block lots of activities of the immune system, especially those making antibodies,” Wherry said. “These would be things like rituximab [which in addition to treating cancer, is used to treat autoimmune conditions like rheumatoid arthritis].”
“Then you have things like removing the muffler, or taking away a couple of doors in the car, things that are much more specific to certain functions of the immune system. And they tend to allow some aspects of the immune system to continue to work, but key pathways that are important in very specific disease processes do not work. This is the case for some of the newer drugs for psoriasis,” he said. “So the level of impact on the vaccine response may be a lot less in those cases because you’re not taking out sort of the main engine of the immune system. You’re taking out an optional component that you would need for one activity, but not others.”
There are no specific studies yet that look at what Wherry calls “more specific immunosuppression regimens.” But there’s some data emerging on the medications that are predicted to have the most broad and dramatic impact on vaccines, he said.
“So right now, I think those more specific things like TNF blockers and some of the other pathways mentioned are less likely to have an all-or-not effect on vaccine responses,” Wherry said. “But the data is emerging very quickly. We’re seeing reports almost daily as we move forward. So, I would stay tuned. I would stay in touch with your physician. But with those drugs, I would be less concerned than some of the other broader immunosuppression situations that we talked about earlier.”
“How many vaccinated immunocompromised people have become ill with COVID. Is there any data on this?”
There have been a couple of studies about breakthrough COVID-19 cases among vaccinated transplant recipients.
Columbia University studied 904 kidney and pancreas transplant patients who got the vaccine. Thirteen of them contracted COVID-19, and seven of those cases met the CDC definition of a breakthrough infection. A similar study from Yale studied solid-organ transplant recipients, and found breakthrough infections occurred in three of 459 fully vaccinated patients.
“Living with an immune deficiency is terrifying. I took the first vaccination, Moderna, and had an awful reaction that took weeks to recover from. I am conflicted when it comes to deciding to take the second shot. What does science tell us about this?”
Side effects like fever, chills, and muscle aches are common, and can be a sign that your immune system is responding. They usually resolve after a day or two, but some people can experience persistent side effects. Adverse events like blood clots, on the other hand, are unexpected reactions to a vaccine.
Wherry said it’s important for this individual to get a second dose. Vaccine clinical trials show people get reasonably good protection after one dose. But the clinical trials do not explain how long that protection after one dose lasts, because everybody in the clinical trials got second doses.
“So it is worth considering getting the second dose at some point down the road. It’s worth talking to your physician,” Wherry said. “It’s possible to get antibody testing in some places, and that might help make that decision about whether or not to get the second dose.”
Most of the side effects pale in comparison to the symptoms of COVID-19, Pereira added.
“So for this particular individual, it really depends on the kind of side effects that they had. But in general, they should proceed with the second scheduled dose,” he said. “Whether they want to delay it for a week or two, they can talk to their provider and discuss some strategies. Certainly after the second dose they can get ibuprofen or acetaminophen to perhaps reduce some of the side effects, but it really depends on the kind of symptoms this person is having.”
I have fibromyalgia and IBS [irritated bowel syndrome]. I don’t take any medication for these. Since the second Pfizer shot, I’ve been having lots of leg, back and overall pain. My joints hurt all over too. Can this be related to the shot?
It could be, or it might not be, both experts said.
“As we’ve vaccinated hundreds of millions of people, everybody is more aware of things that happen at a similar time as getting the vaccine. And so we call this observation bias, or whatever you want to say, that if you watch 100 million people very carefully for a month, you will find events happening even if you don’t vaccinate them,” Wherry said.
“And I’m not saying that that’s the case for this individual. But the temporal link may not be sufficient to infer causality. It may not be unrelated either. It’s hard to know, and especially in individual cases, it’s very hard to ever know causality.”
Pereira said when it’s difficult to tease out the side effects from the vaccine versus symptoms from other chronic illnesses, it might help to note the timing of the symptoms. Side effects usually occur within a few hours to a few days after the vaccine.
“I have several autoimmune conditions, and I am unsure if it will trigger them into flares doing the vaccine.”
Pereira and Wherry said they have not seen any detailed reports showing that autoimmune symptoms worsen following vaccinations. In fact, since many patients with other immune diseases are on some form of immunosuppression, that likely blunts the vaccine responses slightly and may counteract any potential exacerbation that may occur, Wherry said.
“I’m on medication for MS [multiple sclerosis]. My research study team told me for years to stay away from any vaccines. They just don’t know how it might affect my body while on this drug. Can there be adverse vaccine effects for people like me on Kesimpta for MS?”
There are at least 16 different treatments for MS, Wherry said, and their effects on vaccines can vary. Most should only make the vaccine response suboptimal, he said, and it’s unlikely to complicate MS.
The University of Pennsylvania has begun studying which MS medications reduce vaccine effectiveness, and at least one of the drugs does.
Most physicians recommend either getting vaccinated before you start your cycle of treatment for MS or doing it in between cycles, Wherry said.
The National MS Society recommends that if you are about to start Kesimpta, consider getting fully vaccinated two to four weeks or more prior to starting the treatment. There’s no data to guide timing for those already taking Kesimpta. When possible, resume Kesimpta injections two to four weeks after getting fully vaccinated.
Pereira said this individual should probably get the vaccine, without having any expectations of a strong antibody response.
“But again, the immune system is a complex set of cells. And it may be that this person’s T cells will maybe pick up the slack and form some sort of response. So it certainly seems safe. And to get these vaccines, and whether it’s going to be effective or not, it will be a little bit up in the air,” he said.

Saba Tedla, owner of Booker’s restaurant in West Philadelphia, said she’d like to keep their outdoor seating permanently. (Kimberly Paynter/WHYY)
“My husband is 71 and has taken Humira for psoriatic arthritis for 30 years. His daughter and her family are not getting vaccinated. We canceled our trip to visit her. We were planning a three-week stay at her house. Can we ever go there safely?”
Pereira said the public health initiative should focus on understanding why some people don’t want to or are not getting vaccinated. If the husband’s family got vaccinated, they would not only protect themselves against the virus, but also their immunocompromised family member. Until they get vaccinated, they could harbor the virus without knowing it, and transmit the virus to him.
Pereira added that he doesn’t believe Humira affects the immune system that much, but that this individual’s husband should wear a mask, social distance, and avoid being exposed to unvaccinated individuals.
Wherry said these situations will arise more and more.
“I think the real goals here are to get to a high enough level of nationwide vaccine coverage that we eliminate pockets of continued spread or even increases. We’re now starting to see variant virus numbers increase in some places in the U.S., and it correlates very, very well with lower vaccine rates. And so there is a direct correlation between the safety of people at risk visiting with relatives and friends and the coverage rate of vaccination,” he said.
“So as much as there’s, in some parts of the country, a debate about whether they should get vaccinated or not, the data is super clear: When the vaccination rates are lower, the risk of virus spreading is higher.”
A person from Monmouth County asks: I did not develop COVID antibodies, likely because I am taking Rituxan for RA. I am also on IVIG [intravenous immunoglobulin] every three weeks. Can I be around my 11-year-old twin granddaughters whose parents are vaccinated in the house?
These questions come down to risk assessment, both experts said: Consider COVID-19 cases in your location, including the Delta variant of the virus, as well as your grandchildren’s school’s policies around preventing the spread of the coronavirus.
“So we should see vaccination become available for younger kids, or when these 11-year-olds turn 12, they can get vaccinated. These are things that will be changing rapidly over the next four to six months,” Wherry said.
“Locally in the Philadelphia area right now, COVID cases are pretty low, our hospitalization rate is the lowest it’s been in a long time, the rates of local spread are pretty low. The risk may be on the relatively low side. Other parts of the country where you’re seeing continued increase in the rate of spread and new infections, that equation makes it a little bit different.”
“I am immune-compromised from cancer, and have been fully vaccinated. Can I safely be around people who had mild COVID and are not vaccinated?”
“I would say don’t tempt fate,” Pereira said. “The vaccines are not 100% effective. I think if there is an opportunity to avoid that exposure, I would by all means avoid it until they are no longer considered contagious.”
If it’s necessary to be around those with COVID-19 diagnoses, such is the case for health care providers, wear a mask and maintain a physician distance.
Spending time with people who aren’t vaccinated but who don’t have known COVID-19 takes a risk assessment evaluating COVID-19 rates in the area, and whether the unvaccinated people could potentially have the virus due to their daily interactions, Wherry said.
A person from eastern Montgomery County wrote in: “I’m immunocompromised and vaccinated but concerned about going back to the office where there are maskless and unvaccinated people. My company has a mask requirement, however not fully following through on that. How do I cope with this moving forward?”
Wearing a mask yourself, and maintaining a physical distance from others, goes a long way, the experts said. But Pereira added that if you feel comfortable, talk to human resources about your situation. Perhaps they will allow you to work remotely or have your own office space. If comfortable, you can also explain to coworkers that you’re not as protected as other people.
“It’s going to be a tricky situation because on the one hand, you might not want to divulge your medical history, but this is a situation where it is better to be safe than sorry and avoid transmission,” Pereira said. “I think that we’re in a good situation right now that cases are very low and the risk is low overall. But I think it’s probably a good idea to discuss this in advance with the company and figure out ways to avoid that risk.”
WHYY is the leading public media station serving the Philadelphia region, including Delaware, South Jersey and Pennsylvania. This story originally appeared on WHYY.org.

A collection of interviews, photos, and music videos, featuring local musicians who have stopped by the WITF performance studio to share a little discussion and sound. Produced by WITF’s Joe Ulrich.