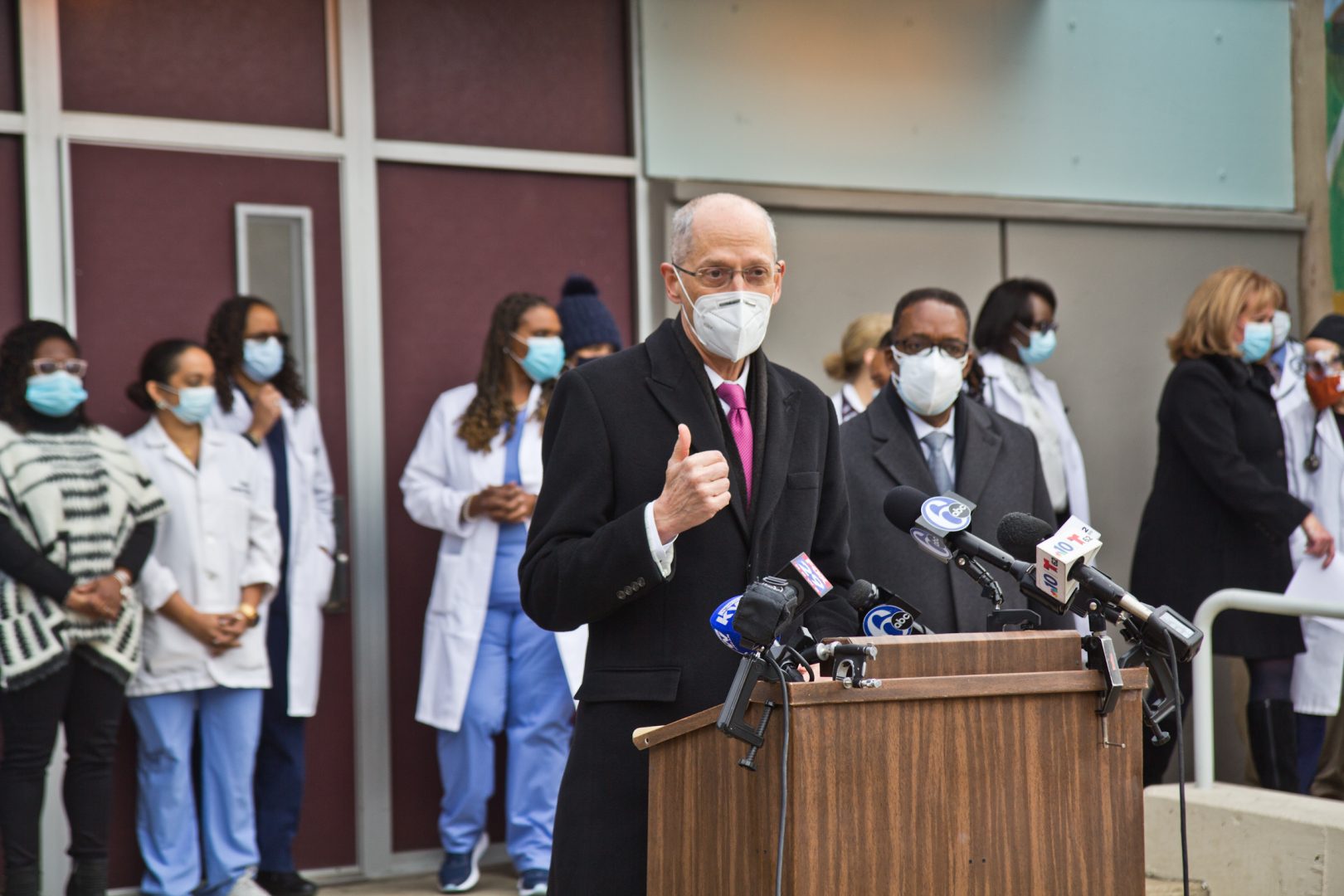
Philadelphia Health Commissioner Dr. Thomas Farley talks about COVID-19 vaccine distribution at a press conference announcing the opening of a vaccine clinic at the city’s Health Center 5 in North Philadelphia Wednesday.
Kimberly Paynter / WHYY
Philadelphia Health Commissioner Dr. Thomas Farley talks about COVID-19 vaccine distribution at a press conference announcing the opening of a vaccine clinic at the city’s Health Center 5 in North Philadelphia Wednesday.
Kimberly Paynter / WHYY
Kimberly Paynter / WHYY
Philadelphia Health Commissioner Dr. Thomas Farley talks about COVID-19 vaccine distribution at a press conference announcing the opening of a vaccine clinic at the city’s Health Center 5 in North Philadelphia Wednesday.
This story is from The Pulse, a weekly health and science podcast from WHYY. Subscribe on Apple Podcasts, Spotify or wherever you get your podcasts.
I remember very clearly the day I stopped totally trusting my city’s health commissioner. It was the last Tuesday in July of 2020, during a virtual press conference I was attending.
Philadelphia’s Department of Public Health had been doing pandemic briefings for months at that point. Health Commissioner Dr. Thomas Farley always popped up to do his rundown of the state of the virus for the week. This press conference was no different.
Except after the numbers and talk about trends, Farley said this: “So in summary, the second wave of the epidemic has now reached Philadelphia.”
And I just plain didn’t believe him.
The second wave was supposed to be the big one — federal health officials had warned it could dwarf the initial spring COVID-19 outbreaks. But Farley’s evidence seemed flimsy to me.
Basically, he made the case that “southern states reopened too quickly and too recklessly. There’s a second wave that started there and then is spreading north and east from there. That wave has now just arrived in Philadelphia.”
It seemed like nonsense to me: The virus sweeping across the country geographically like a physical, literal wave? I looked for some kind of data mapping that could back this up, and couldn’t find anything.
The numbers didn’t seem right either. Positive cases were up significantly, sure, but so too was testing. I did the math from the raw numbers Farley gave: Both testing and positive cases had gone up 47% precisely. That would indicate the situation was more or less stable — we were just detecting more of the virus that was always present.
But Farley stayed on this second wave idea, announcing indoor restaurant restrictions would have to continue. “The second wave has simply hit us right now,” he said.
His announcement lit up the airwaves, everyone had the same headline, some version of: Second wave of COVID is here. I didn’t feel comfortable writing a headline like that, so instead I emailed a Health Department spokesperson with a long fact-check that amounted to: I don’t buy it. There’s not much evidence the second wave has hit, that there even is one.
The spokesperson sent me a lengthy response, and the part that really struck me was right at the end. He said the media wants to point to an “impressive graph with rapidly rising cases to show people cases are rising.”
“Public health officials, however, have a vested interest in keeping those case counts as low as possible, so we never have to show one of those graphs again. Dr. Farley is warning people that we are starting to see hallmarks of a second rise in cases, and he’s doing everything in his power to stop that from happening,” the email continued. “We would rather call a slight rise in cases the start of a second wave than wait too long and have to deal with uncontrollable spread.”
A slight rise in cases? Hallmarks of a second rise in cases?
That sounded a lot different from what was said in the press conference to everybody else. It sounded to me like the Public Health Department was saying a second wave was here in order to scare people into behaving cautiously enough to avoid a true second wave.
I wanted a headline that said something like ‘No evidence for a second wave.’ The editor, though, went with “Is Philly experiencing a second wave?” (A little inside baseball: When a news headline asks a yes or no question, the answer is almost always no.)
I was pretty nervous about this at the time, like who am I to question the head of a major American city’s health department? To question a scientist protecting us from the pandemic?
But, as it turns out, I was right.
I asked Farley about this summer second wave at a later press conference, in September.
“Well, I definitely called it wrong,” Farley said. “Because I said that the case rates were likely to rise and they didn’t rise … they fell.”
There really was no second wave.
I asked did he worry his summer announcement would harm his credibility if a true second wave hit in the late fall or winter?
“As I said, I call it wrong then,” he said. “I think the lesson is that this is very unpredictable.”
That’s not the lesson I got.
I still believed COVID-19 was real, believed in masks and social distancing and all that. But I no longer believed our public health department — not completely.
Why speak with such certainty, with so little evidence, about something so scary? Was it a message we needed to hear to cancel that innocent get together with just a few friends?
I wondered if this kind of framing, truth-shaping to nudge us in one direction, was this just a part of public health?
Peter Sandman is a veteran risk communication expert — he was one of the academics that essentially created the field in the 1980s. I asked him about my experience.
“There are a lot of things about this pandemic that haven’t happened in a hundred years, but public health being misleading in order to get people to do the healthy thing? That’s not unique to this pandemic,” he said. “That’s absolutely typical.”
Sandman is retired now, sort of.
“By 2019, I was completely retired and then early in 2020, when COVID-19 reared its ugly head, it looked like a stupid time to be retired given that that’s something I worked on,” he said. “I’d worked on bird flu, I’d worked on swine flu. I’d worked on Zika. I’d worked on Ebola. It seemed stupid not to come back for COVID-19. So, I un-retired.”
Sandman has had a decades-long career as a risk communication consultant and academic working for all manner of big-name environmental, public health, government, and corporate outfits. Everyone from the Nuclear Regulatory Commission to the World Health Organization, from ConocoPhillips to Procter & Gamble.
Over the years, he said, he’s noticed something about the folks he calls the good guys, the nonprofits and governmental organizations with good-for-society, altruistic goals — people like those in public health: They don’t mind exaggerating the case for their cause here and there.
They’re the good guys after all, their goals are good. They’re not trying to make a buck, they want to save us.
“You don’t feel like you’re misleading. You feel like you’re saving lives, you know,” he said. “And you are saving lives, and you are misleading. And the most interesting question, is that ok? Do we want a world in which public health people say things that aren’t strictly true when in their best judgment doing so will lead to better health outcomes?”
That’s been the big question of the pandemic for guys like Sandman. For governments and scientists, it’s been a yearlong exercise in critical global risk communication, and the stakes have maybe never been higher.
When Sandman talks about less-than-truthful public health messages, he’s referring most often to this one — in his mind – regrettable practice: “They gild the lily,” he said.
Gilding the lily means needlessly trying to improve an already good thing. He offered an anti-smoking example.
“One of the things that the Cancer Society endlessly says is corporations ought to do anti-smoking programs because your employees smoke, they get lung cancer, and that costs you a lot of money,” Sandman said.
He used to be on a public information committee for a state chapter of the American Cancer Society. At one point, they looked to an economic analysis to quantify how much money smoking employees cost their companies.
The problem: The analysis showed smoking could actually save employers money. Smokers died earlier than nonsmokers, so there were fewer years of medical coverage and pension payments.
“It’s grim, yeah, but it wasn’t like we were going to stop urging people to quit smoking, ’cause we want people to live as long as possible,” Sandman said. “But we should have stopped telling corporations that it was in their self-interest, because we had learned that it wasn’t.”
Cancer Society literature does still argue smoking cessation saves corporate money. To Sandman, it’s an example of gilding the lily. He thinks the perfectly true argument that smoking greatly increases your risk of a slow and painful death is powerful enough on its own.
Why stack the deck?
“They don’t trust the public,” Sandman said. “They think if you give a balanced argument, the public’s likely to screw it up. and the best way to get the public to make the right decision is to pretend it’s a no-brainer, and there’s no decision to be made.”
But gilding the lily has risks. Sandman said that’s become painfully obvious during the pandemic.
Take the messaging about masks early in 2020. At that time, public health agencies knew for certain that hospitals would start running out of personal protective equipment. They also knew asymptomatic spread of the virus was possible.
“But they genuinely didn’t know how often it happens,” Sandman said.
It was an unknown. Masks might be useful for the public or might not, nobody really knew for certain.
“But that’s not what they say, what they said is, ‘Masks are useless in ordinary life,’” Sandman explained.
The former U.S. surgeon general actually said it in using caps lock: “STOP BUYING MASKS!” He said in a now-deleted tweet from Feb. 29, 2020: “They are NOT effective in preventing general public from catching #Coronavirus.”
A more balanced message would have been: Social distance, stay home, and you’ll be safe enough. Don’t buy masks because hospital workers need them more right now.
The added messaging about the uselessness of masks — what fuels a great deal of mask denial to this today — that’s a gilded lily, Sandman said.
It’s still happening with vaccines, he said. You may have heard that the top three — Pfizer, Moderna, and Johnson & Johnson — are all 100% effective against death from COVID-19.
“You know, that’s true in the sense that in all three Phase 3 trials, nobody who was fully vaccinated after the period of time, when the vaccine kicks in completely, nobody died,” Sandman said.
When I talked to Sandman, it was after I had lucked into a super-early vaccination. My hospital just called me in out of the blue — I felt like I won the lottery. One hundred percent death-proof sounded great to me.
“But in the placebo groups, almost nobody died. I’m looking at the numbers here. I’ll give you the Pfizer number. Cause that’s the most stunning,” said Sandman. “In the vaccine group, nobody died; in the placebo group, also nobody died. So the argument that the Pfizer vaccine prevented death is exactly as strong as the argument that the pleaser placebo prevented death.”
There were actually some deaths in the placebo group, just from causes unrelated to COVID. So I was admittedly less jazzed about my ironclad vaccine after hearing that — and kind of stunned I somehow didn’t know this already.
“There’s nothing wrong with the vaccine. There’s nothing wrong with the trials. There’s something wrong with the sales pitch,” Sandman said.
The vaccines are highly effective. The reason the placebo group and vaccine group were so close is because the trials were so unusual. They didn’t run for that long — Operation Warp Speed and all — plus we were all social distancing and wearing masks while it was going on, really abnormal life patterns. Fewer people got the chance to be exposed to the virus and potentially die from it than may have been exposed to Disease X during another, longer vaccine trial pre-pandemic.
So should public health be touting the vaccines as 100% effective against death from COVID? And if they didn’t say that, would so many people still be lining up, so eager for an experimental shot on emergency use approval?

Matt Rourke / AP Photo
Members of the military inoculate people with the Johnson & Johnson COVID-19 vaccine at the Esperanza Community Vaccination Center in Philadelphia, Friday, April 9, 2021.
Holley Wilkin is a health communications professor at Georgia State University. I asked her about this message — that vaccines were 100% effective in preventing COVID-19 death, when the placebo had the same result as the real thing when it came to that.
Isn’t this misleading? Is it wrong?
A little, she said, but with a caveat.
“We want to go back to living, presenting it in the simplest, most basic form, that’s going to get the most people to do the recommended health behavior now,” Wilkin said. “We believe that it’s going to have the biggest impact if we get more people vaccinated now.”
As I began writing this article in March, the virus was surging again in parts of Europe, where for mainly logistical reasons the vaccination rate was much lower than here. I saw a headline about intubations in a packed hospital parking lot in Greece.
Here in the states more recently, the experts have been worrying that not enough people will get the shot for true herd immunity. Demand has waned.
So Wilkin does have a point.
Wilkin trains future public health officials. It occurred to me that I didn’t really know anything about them, or about their jobs, pre-pandemic. I had been thinking of public health as a kind of objective scientific organ: Data and science tell us this and that — and, on such and such basis, we’re now telling you this.
Can you really blame me? They’re always saying they’re following the science, and that the data is making the decisions.
But Wilkin said it’s always been more complicated than that. Like Sandman, she explained with a smoking example.
“So we think of something like smoking, and most people think, ‘Oh, well, everybody knows that it’s bad for you,’” she said. “Well, at what point in your life did you figure out that it was bad for you? And had they successively already convinced you to try smoking before then?
“They” being Big Tobacco.
“They’re out there using persuasive messages, and they have big marketing budgets,” she said. “And so, with very considerably smaller budgets, public health people have to figure out, OK, how do we counter those arguments that are out there.”
To essentially punch above its weight class, public health has to arm itself with more than just the plain and whole truth. It has to use what Holley calls “appeals.” Precisely speaking, she means emotional appeals. They can be to sadness, to empathy, to guilt, but most often they’ve been appeals to fear.
A classic example is the old your brain on drugs ad, where a matter-of-fact-looking guy pulls out an egg.
“THIS IS YOUR BRAIN,”
And a hot pan …
“THIS IS DRUGS … ”
And combines the two:
“THIS IS YOUR BRAIN ON DRUGS,
He fries the egg, your brains.
“ANY QUESTIONS?”
The ad doesn’t really tell you anything about addiction, how it develops, or how drugs work or that they can be pretty fun, at least for a while. It just tells you drugs will destroy you.
Fear can be very persuasive.
“I had a doctor once tell me that, you know, communicating with patients isn’t difficult at all. ‘I just tell them they’re going to die if they don’t take these meds, and they do it,’” Wilkin said.
The fear appeal can work quickly, but Wilkin thinks public health has leaned on it too much for too long during the pandemic.
She discourages the fear appeal in general, she said, because studies have found it unpredictable: You never know how it’s going to break, who it will work on, and for how long.
Some people get scared and stay scared; some people get defiant. You end up with the battle cry of the anti-masker, which isn’t “I don’t care about Grandma.” It is, quite tellingly, “I refuse to live in fear.”
“We have what we call … a third-person effect, where you don’t necessarily believe the media is impacting you, but you believe other people would be impacted by particularly things that they see or they hear in the media,” Wilkin said. “The fear appeal is very much like that.”
Fear also appeals to news organizations. If it bleeds it leads, and Wilkin said public health officials understand this. A fear appeal may get you headlines, while another kind of appeal won’t.
“People might not be tuning into the press conferences anymore,” she said. “At a certain point, I think people no longer start to see the human element, that they start to see you just having these increasing numbers.”
I mentioned the Philadelphia press conference I had covered — the one about the second wave hitting, and that a lot of media outlets ran that. What would the headlines have been if the health commissioner had just said a slight rise in cases, keep an eye out? Would there have even been any headlines?
At that summer press conference, Farley didn’t announce any new public health measures to go with the second wave announcement, but he also didn’t remove any. Some restrictions were slated to be relaxed the next week, and they were extended.
Wilkin, however, said that just talking about a second wave was an active public health measure in and of itself. Just saying those words on TV, that can save lives.
“What we’re seeing now is this is really being spread, within families and in social events,” Farley had said later in that July summer second-wave press conference. “And so we’re making a recommendation today to try to limit exposure, then to families and social events.”
What public health measure gets people to stop seeing their own families, especially during beautiful summer days, and after months apart? Maybe it’s pulling the trigger on a fear appeal, a big one, like a second wave.
To help me better understand Farley’s situation, Wilkin gave me an example from when she was a kid.
“When I was in middle school, we had to do a game in our science class where each day we got to check the seismic readings around Mount St. Helens and had to make a decision on whether or not you’re going to evacuate the town or not,” she said.
Too early and people lose confidence in you — we left and nothing happened. But make a move too late …
“And now you’re dealing with a bunch of people who have died as a result of you not acting soon enough,” she said. Either way, “Everybody who’s around knows you made the right call or you didn’t make the right call because an actual volcano explodes.”
With pandemic public health, if you do everything right, the volcano never goes off. All is quiet when a crisis is averted — which can make prevention measures seem like total overkill.
There is a possibility that Farley’s simply saying that there was a second wave last summer did something to stave one off. There really is no way to know.
Farley declined to be interviewed for this story, but I really wish he would have. I wrote to his spokesperson, saying that I wanted to know what I didn’t know, the factors he weighed behind closed doors before deciding to declare a second wave, the pressures he felt.
I don’t know what it’s like to be in his position, to make life-and-death decisions, even if indirectly, for an entire city. There’s a strong case he did gild the lily, but he definitely saved more lives than I have this past year.
The question then becomes at what cost.

Kate Landis / PA Post
FILE PHOTO: A woman holds an anti-mask sign at a May 15, 2020, ReOpen PA protest outside the state capitol in Harrisburg, Pa.
I live in a deep blue city, run in progressive circles, most people I know want to believe the Farleys of the world.
But what about others? People who don’t trust experts or officials, who believe COVID conspiracies, or think the virus is no worse than the flu, a ploy to control us?
Sandman, the expert on risk communication, said gilding the lily, overstating some things while keeping quiet about others, can become jet fuel for misinformation and conspiracy theories.
“Let’s take vaccination, for example. The easiest way to find out the small percentage of the truth that’s genuinely anti-vax is to read anti-vax websites, and you have to wade through a lot of falsehood, but you’ll also find the little pieces of truth that public health is pretending don’t exist,” he said.
What if, instead of Sandman telling you a clinical trial found no difference between the placebo and the vaccine in terms of COVID deaths, it’s someone ranting on YouTube. He’s red in the face, screaming all kinds of scary nonsense, but then he says something about Pfizer that a) is true, b) is kind of troubling, and c) that no mainstream authority has bothered telling you.
How does that change who you believe? And who you trust?
But that’s maybe a peacetime concern. We’re still in a war against this virus. It’s hard to know the right move, especially when dealing with imperfect, irrational humans.
Throughout this story, I’ve really been asking two questions: How much can we trust public health? And how much does public health trust the public, trust us?
But Wilkin brought up a third, harder question: How much trust does the public deserve?
We were talking about masks.
“I have friends that live in the U.S. but were born in China or in other places in Asia,” she said. “And they were all going, ‘Oh my God, why are they not telling us to wear face masks? Face masks help!”
She started to say the messaging should have been straightforward, no appeals at all, just the complicated reality. But then she remembered toilet paper. The way we all lost our minds scrambling for it, and cleaned out the store shelves.
“Was the rationale that they were afraid that people are going to hoard the face masks? Like they hoarding toilet paper?” she asked.
It’s nice to think we would have all banded together in a patriotic, scientifically informed fervor to protect our meager mask supply. But honestly I doubt we would have — we’re the country of Black Friday sale stampedes after all. Ammunition sales spiked right alongside toilet paper.
And Sandman said there is a hazard in trusting the public with too much science. They realize it’s imperfect. That it can be, and is wrong, all the time.
Still, he’s settled on honesty is the best policy — the whole truth, warts and all, as often as you can.
“It’s my argument in the longer term that the lives they saved by misleading us are not worth it because their credibility is at stake, and they should be honest, even at the cost of their campaigns being less effective,” he said. “That’s my opinion. I cannot prove it. I don’t have good data.”
If the COVID-19 pandemic truly is once in a century, maybe public health gets away with lily gilding and fear appeals stretched too far.
By the time the next pandemic comes along, maybe all anyone will remember is science saved everyone, and miracle vaccines in record time.
But if that’s not the case, as some epidemiologists predict, Sandman said that above honest public health, above trustworthy and transparent public health, what’s most important now is accountable public health.
“Don’t ask to be trusted. Don’t want to be trusted. What you should want to be is accountable, more than trust,” he said. “What we need is accountability.”
I am thankful for the efforts Farley and others in public health have made this past terrible year. They choose to serve, to try to protect the health of their communities — to protect me. I know that impulse is likely behind every decision, right or wrong.
But, as for me, I won’t believe or not believe everything Farley says.
I’ll treat him like a reporter should treat any city official talking from behind a podium. I’ll listen, but with a healthy dose of adversarial, respectful doubt.
Sometimes, your mornings are just too busy to catch the news beyond a headline or two. Don’t worry. The Morning Agenda has got your back. Each weekday morning, host Tim Lambert will keep you informed, amused, enlightened and up-to-date on what’s happening in central Pennsylvania and the rest of this great commonwealth.